ORIGINAL ARTICLE
PREDICTORS OF PHYSICAL AND PSYCHOLOGICAL VIOLENCE AMONG COMMUNITY-DWELLING ELDERLY PEOPLE
PREDICTORES DE VIOLENCIA FÍSICA E PSICOLÓGICA ENTRE PERSONAS MAYORES COMUNITARIAS
PREDITORES DE VIOLÊNCIA FÍSICA E PSICOLÓGICA ENTRE PESSOAS IDOSAS COMUNITÁRIAS
https://doi.org/10.31011/reaid-2024-v.98-n.3-art.2128
1Gleicy Karine Nascimento de Araújo-Monteiro
2Rafaella Queiroga Souto
3Rute Costa Régis de Sousa
4Renata Clemente dos Santos-Rodrigues
5Izabel Cristina Brito da Silva Carvalho
6Anna Luiza Castro Gomes
7Bárbara Maria Lopes da Silva Brandão
1Universidade Federal de Alagoas, Maceió, Brasil. Orcid: https://orcid.org/0000-0002-4395-6518
2Universidade Federal da Paraíba, João Pessoa, Brasil. Orcid: https://orcid.org/0000-0002-7368-8497
3Universidade Federal de Pernambuco, Recife, Brasil. Orcid: https://orcid.org/0000-0002-2670-2620
4Universidade Estadual da Paraíba, Campina Grande, Brasil. Orcid: https://orcid.org/0000-0003-2916-6832
5Universidade Federal de Pernambuco, Recife, Brasil. Orcid: https://orcid.org/0000-0001-6410-9919
6Universidade Federal da Paraíba, João Pessoa, Brasil. Orcid: https://orcid.org/0000-0002-5551-0468
7Universidade Federal da Paraíba, João Pessoa, Brasil. Orcid: https://orcid.org/0000-0002-6652-9615
Corresponding author
Bárbara Maria Lopes da Silva Brandão
Cidade Universitária, s/n - Castelo Branco III, João Pessoa - PB, 58051-085, Brasil. +55(81) 997394470. E-mail:
Submission: 02-01-2024
Approval: 16-06-2024
ABSTRACT
Objective: to identify the predictive factors of physical and psychological violence among community-dwelling elderly people. Methods: cross-sectional study, household survey was carried out with a representative sample of elderly people registered in a Family Health Unit, located in a Health District of Recife City, Pernambuco, in the period from 2016 to 2017. Descriptive, bivariate (Pearson's chi-square, and Fisher's exact test), and multivariable logistic regression were used to test the relationship among the variables. Results: psychological violence presented higher frequency, associated with the variables: being married or living together, suffer from urinary incontinence, and having someone to care for them if they got sick. Conclusion: living together or being married, suffering from urinary incontinence, and having someone to care for them in case of illness were presented as predictors of psychological violence among community-dwelling elderly people. For physical violence, the associated factors were having a paying job, and existence of depressive symptoms.
Keywords: Nursing; Forensic Nursing; Geriatric Nursing; Exposure to Violence; Aged.
RESUMEN
Objetivo: identificar los factores predictivos de violencia física y psicológica entre personas mayores comunitarias. Métodos: estudio transversal, con amuestra representativa de personas mayores catastradas en una Unidad de Salud de Familia, situada en un distrito sanitario de la ciudad de Recife, Pernambuco, durante el periodo de 2016 a 2017. Resultados: fue identificado una alta frecuencia de violencia psicológica, asociada con las variables de estar casado o viviendo con alguien, tener incontinencia urinaria, y tener alguien para cuidar cuando la persona está enferma. Conclusión: vivir con alguien o ser casado, sufrir de incontinencia urinaria y tener alguien para cuidar en caso de enfermedad fueron considerados factores predictivos de violencia psicológica en personas mayores. Para violencia física, los factores asociados fueron tener un trabajo remunerado y demonstrar síntomas depresivos.
Palabras-clave: Enfermería; Enfermería Forense; Enfermería Geriátrica; Exposición a la Violencia; Anciano.
RESUMO
Objetivo: identificar os fatores preditivos de violência física e psicológica entre pessoas idosas comunitárias. Métodos: estudo transversal, com amostra representativa de pessoas idosas cadastradas em uma Unidade de Saúde da Família, localizada em um distrito sanitário da cidade de Recife, Pernambuco, durante o período de 2016 a 2017. Estatística descritiva, bivariada (teste qui-quadrado de Pearson e exato de Fisher), e regressão logística multivariada foram utilizadas para testar a relação entre as variáveis. Resultados: foi identificado uma alta frequência de violência psicológica, associada com as variáveis estar casado ou morando com alguém, sofrer de incontinência urinária, e ter alguém para cuidar quando estiver doente. Conclusão: morar com alguém ou ser casado, sofrer de incontinência urinária e ter alguém para cuidar em caso de doença estiveram presentes como fatores preditores de violência psicológica em pessoas idosas comunitárias. Para violência física, os fatores associados foram ter um trabalho remunerado e demonstrar sintomas depressivos.
Palavras-chave: Enfermagem; Enfermagem Forense; Enfermagem Geriátrica; Exposição à Violência; Idoso.
INTRODUCTION
It is estimated that approximately 15.7% of the elderly population are subject to abuse situations. This number may be underreported since the secrecy surrounding this phenomenon masks the actual data(1). Elder Abuse (EA) is a pervasive phenomenon that has devastating effects such as decreased quality of life, increased morbidity, mortality and hospitalization rates(2).
Being a vulnerable population, elderly people, have been identified as a priority to the International Association of Forensic Nursing (IAFN) research agenda(3). Thus, Forensic Nursing (FN) as a link between the forensic health sciences and the legal sector could play an important role in prevention and control of EA(4).
The World Health Organization (WHO) defines EA as "a single or repeated act or lack of appropriate action occurring in any relationship where there is an expectation of trust that causes injury or suffering to an elderly person", that either results from intentional negligence or not and expresses itself on the forms of physical, psychological, financial or sexual abuse, and neglect(1).
Abuse is comprised of acts committed in different spaces and social contexts, and it is perpetrated by distinct aggressors, making it necessary to obtain a broader analysis of its diverse typology, as well as the profiles of its victims and aggressors(6). Abuse is also associated with an increased risk of mortality and hospitalization while its clinical manifestations are hard to identify and vary among the different subtypes of abuse(7).
Intrafamily violence refers to acts committed by family members or intimate partners, of which the elderly person becomes more and more susceptible to its occurrence as the dependence level rises(8). Strained relationships developed in the family environment, combined with the vulnerability of the aging process, make the scenario susceptible to the emergence of violent and conflicting interactions related to health, social relationships, care needs, financial issues, or family coexistence(9).
Undoubtedly, the growth in the number of older people around the world is a reality. In Portugal, it is estimated that by 2032, the number of elderly people aged 80 or over might double the number of young people(6). This progress is followed by an increasing rate of elderly victims of abuse, bearing in mind that Portugal is ranked by WHO as one of the five countries with the worst living conditions for this age group(1).
Social and gender relations also feature as important determinants of EA occurrence. A study developed concomitantly in Canada, Colombia, Albania, and Brazil found that family arrangements and low social conditions are associated with EA and that elderly women were 1.8 more times more likely to experience psychological abuse(10).
Nurses should use already validated instruments to screen for intrafamily violence. The Conflict Tactics Scale - 1 (CTS-1) is a scale for measuring occurrence of family violence including physical and psychological violence, both objects of the present study.
Psychological abuse is characterized by all forms of discrimination, humiliation, prejudice and contempt that results in feelings of isolation, sadness, loneliness, and depression(11). The higher prevalence of psychological abuse when compared to other types of violence, discussed in the literature, has found that psychological usually precedes physical abuse(12).
Physical abuse is the most evident form of abuse and can result in body injuries demanding victim hospitalization, it may be defined as the use of physical force to coerce someone to submit to undesired situations that causes suffering, pain, incapacity or death(8,10).
A systematic review of the prevalence of EA in Asian studies identified these risk factors: age, gender, marital status, educational level, income, physical health, and cognitive ability(13). Systematic screening for risk factors and indicators of EA are critical to detection and early prevention of this problem, enabling a better professional performance of health personnel.
Despite the ever-growing number of elderly people in Brazil, the issue of EA only came to be addressed in the last two decades. Elder abuse is multi-faceted and complex, thus has not been well researched(14). Finding the predictive factors for EA occurrence is extremely relevant to consolidate FN in Brazil, as well as for building an evidence-based nursing practice to prevent EA measures and find useful interventions.
In view of that, the purpose of this study was to identify predictors of physical and psychological violence among community-dwelling elders by using a culturally adapted translated version of the Conflict Tactics Scale-1 (CTS-1) in a community-based elderly population(11).
METHOD
We conducted an analytical, cross-sectional, household survey with a representative sample of elderly people registered in a Family Health Unit (FHU), located in the micro area III of the Health District IV of Recife City, Pernambuco, in the period from 2016 to 2017. The study population was 1209 elders (number of elders registered in three teams of the health unit). The sample size was determined by a power analysis based on the finite population formula for epidemiological studies, adopting a confidence level of 95% and standard error of 8%.
Systematic random sampling was used from the register list of elderly people of the health unit, so one from each five elders was chosen and invited to participate in the research. The inclusion criteria were all elderly population registered in the health unit where the research was conducted, which by Brazilian law are those individuals aged 60 years or older. Those who were terminally ill; had severe hearing, visual impairment, or serious cognitive deficit were excluded. These exclusion criteria were applied based on the researcher judgment.
By applying these criteria through researcher’s observation, 17 individuals did not participate in the sample. Participants did not receive any financial incentive to participate in the research. Trained interviewers face-to-face in a private space conducted all interviews. To avoid possible literacy issues the interviewer read out loud all the questionnaires questions.
Similarly, to other cross-sectional studies on violence against the elderly living in the community, psychological and physical violence in the last 12 months was investigated using an adapted version of the CTS-1 tested for reliability and validity in a Brazilian study(11). This screening tool aims to identify cases of violence occurring in the last 12 months. It has 19 questions, divided into three groups, comprised of different kind of strategies used to deal with conflicts: argumentation (items a-c), verbal aggression (items d-f and h-j), and physical aggression (k-s items). Each item has three options: it has not happened, it has happened a few times in the last 12 months, and it has happened several times in the last 12 months. Individuals who answered "it has happened a few times" or "it has happened several times" to any of the comprised in the physical and verbal aggression group were identified as a case of elder abuse(11).
Existence of “depressive symptoms” was investigated using the Geriatric Depression Scale - 15 (GDS-15)(15), that scores as depressive symptoms individuals with a final score equal or greater than five points. Respiratory diseases, urinary incontinence, and foot conditions that compromised mobility were self-reported by respondents.
Living arrangement refers to whether the elderly lived alone or shared the residence with someone. The variable "having someone to care for them in case of illness", addressed the elder person perception that if he/she got sick or had a health decline, someone could stay with her/him in the hospital or provide care at home. Socioeconomic variables included: sex, age, marital status, literacy, work, and income. Physical abuse and psychological abuse were the dependent variables. Independent variables were: sex, age, marital status, literacy, paying job, income, living arrangement, someone to care for them, depressive symptoms, respiratory diseases, urinary incontinence, and foot conditions.
Descriptive statistics (frequencies, Pearson's Chi-square, and Fisher's Exact test) were used to characterize the sample and to test the bivariate relationships between the independent variables and the dependent variables (physical and psychological abuse). Multivariable logistic regression model was used to quantify the relationship among the independent variables and physical and psychological abuse. All independent variables that met the inclusion criterion of p<0.2 in the bivariate analysis were included in the model. Statistical significance was set at p<0.05. Analyses were carried out using SPSS version 23.0.
This research was submitted to the Ethics and Research Committee of the Federal University of Pernambuco for consideration and was approved under number 1413599/16. All recommendations and ethical principles required in research involving human beings were respected and followed in accordance with Resolution 466/12, established by the National Health Council.
RESULTS
Psychological violence was the subtype of EA with the highest prevalence (35.7%, n = 55). Psychological violence showed a statistically significant association with being married or living together (Table 1), suffering from urinary incontinence and having someone to care for them in case of illness (Table 2).
Table 1 - Prevalence of violence subtypes according to sociodemographic characteristics of the elderly in the study. Recife, PE, Brazil, 2016-2017
|
Variables |
Psychological violence |
Physical violence |
||
|
Yes n (%) |
No n (%) |
Yes n (%) |
No n (%) |
|
|
Sex |
|
|
|
|
|
Male |
12 (33.3) |
24 (66.7) |
2 (5.6) |
34 (94.4) |
|
Female |
43 (36.4) |
75 (63.6) |
8 (6.7) |
111 (93.3) |
|
p-value |
0.733* |
1.000** |
||
|
Age |
|
|
|
|
|
≤ 70 years old |
33 (39.8) |
50 (60.2) |
8 (9.5) |
76 (90.5) |
|
>70 years old |
22 (31.0) |
49 (69.0) |
2 (2.8) |
69 (97.2) |
|
p-value |
0.257* |
0.110** |
||
|
Marital status |
|
|
|
|
|
Married/living together |
25 (48.1) |
27 (51.9) |
4 (7.7) |
48 (92.3) |
|
Single/widowed/divorced |
30 (29.4) |
72 (70.6) |
6 (5.8) |
97 (94.2) |
|
p-value |
0.022* |
0.733** |
||
|
Literacy |
|
|
|
|
|
Literate |
38 (36.9) |
65 (63.1) |
7 (6.7) |
97 (93.3) |
|
Not literate |
17 (33.3) |
34 (66.7) |
3 (5.9) |
48 (94.1) |
|
p-value |
0.664* |
1.000** |
||
|
Paying job |
|
|
|
|
|
Yes |
10 (40.0) |
15 (60.0) |
5 (19.2) |
21 (80.8) |
|
No |
44 (35.8) |
79 (64.2) |
5 (4.1) |
118 (95.9) |
|
p-value |
0.689* |
0.015** |
||
|
Income |
|
|
|
|
|
39 (35.1) |
72 (64.9) |
8 (7.2) |
103 (92.8) |
|
|
More than 1 minimum wage |
16 (37.2) |
27 (62.8) |
2 (4.5) |
42 (95.5) |
|
p-value |
0.810* |
0.726** |
||
|
Living arrangement |
|
|
|
|
|
Alone |
8 (38.1) |
13 (61.9) |
1 (4.5) |
21 (95.5) |
|
Living with someone |
47 (35.3) |
86 (64.7) |
9 (6.8) |
124 (93.2) |
|
p-value |
0.806* |
1.000** |
||
|
Someone to care for them |
|
|
||
|
Yes |
43 (32.1) |
91 (67.9) |
||
|
No |
12 (60.0) |
8 (40.0) |
||
|
p-value |
0.015* |
0.619** |
||
* Pearson’s Chi-square Test; ** Fisher’s Exact Test.
Table 2 - Prevalence of violence subtypes according to some health-related factors of the elderly in the study. Recife, PE, Brazil, 2016-2017
|
Variables |
Psychological violence |
Physical violence |
||
|
Yes n (%) |
No n (%) |
Yes n (%) |
No n (%) |
|
|
Depressive symptoms |
|
|
|
|
|
Yes |
17 (44.7) |
21 (55.3) |
5 (13.2) |
33 (86.8) |
|
No |
37 (32.5) |
77 (67.5) |
5 (4.3) |
110 (95.7) |
|
p-value |
0.171* |
0.121** |
||
|
Respiratory diseases |
|
|
|
|
|
Yes |
8 (34.8) |
15 (65.2) |
3 (13.0) |
20 (87.0) |
|
No |
47 (35.9) |
84 (64.1) |
7 (5.3) |
125 (94.7) |
|
p-value |
0.919* |
0.170** |
||
|
Urinary incontinence |
|
|
|
|
|
Yes |
32 (46.4) |
37 (53.6) |
5 (7.2) |
64 (92.8) |
|
No |
23 (27.4) |
61 (72.6) |
5 (5.9) |
80 (94.1) |
|
p-value |
0.015* |
0.754** |
||
|
Foot conditions that compromised mobility |
|
|
|
|
|
Yes |
17 (36.2) |
30 (63.8) |
5 (10.6) |
42 (89.4) |
|
No |
37 (34.9) |
69 (65.1) |
5 (4.7) |
102 (95.3) |
|
p-value |
0.880* |
0.175** |
||
* Pearson’s Chi-square Test; ** Fisher’s Exact Test.
In the logistic regression (Table 3), psychological abuse was more likely to occur in married elderly (OR = 2.92, 95% CI = 1.37-6.19), who suffered from urinary incontinence (OR = 2.74, 95% CI % = 1.32-5.66) and had someone to care for them if they got sick (OR = 3.67, 95% CI = 1.33-10.10).
Physical abuse exhibited a prevalence of 6.5% (n = 10), and statistically significant association with: having a paying job (Table 1). Physical abuse had more probability to happen in the elderly (Table 3) who still engaged in a paying job (OR = 7.87, 95% CI = 1.83-13.73) and had depressive symptoms (OR = 4.97; 95% CI = 1.16-21.18).
Table 3 - Multiple logistic regression of relationship between violence subtypes and elderly characteristics. Recife, PE, Brazil, 2016-2017
|
Variables |
|
OR |
CI |
p-value* |
|
Psychological violence |
Marital status |
|
|
|
|
Married/living together |
2.92 |
[1.37-6.19] |
0.005 |
|
|
Single/widowed/divorced |
1.00 |
- |
- |
|
|
Urinary incontinence |
|
|
|
|
|
Yes |
2.74 |
[1.32-5.66] |
0.006 |
|
|
No |
1.00 |
- |
- |
|
|
Someone to care for them |
|
|
|
|
|
Yes |
1.00 |
- |
- |
|
|
No |
3.67 |
[1.33-10.10] |
0.012 |
|
|
Physical violence |
Paying job |
|
|
|
|
Yes |
7.87 |
[1.83-33.73] |
0.005 |
|
|
No |
1.00 |
- |
- |
|
|
Depressive symptoms |
|
|
|
|
|
Yes |
4.97 |
[1.16-21.18] |
0.030 |
|
|
No |
1.00 |
- |
- |
OR: Odds Ratio; CI: Confidence Interval; * Test Significance.
Table 2 presents the relationship between subtypes of abuse and some health-related factors analyzed by the study. When assessing psychological abuse, we found a significant association between suffering from urinary incontinence and having someone to care for them.
Physical abuse did not show a statistically significant association any variables. But it was the most prevalent abuse subtype among elders with depressive symptoms, respiratory disease, incontinence, persons with some kind of foot conditions that decreased mobility and who had no one to care for them if they become ill.
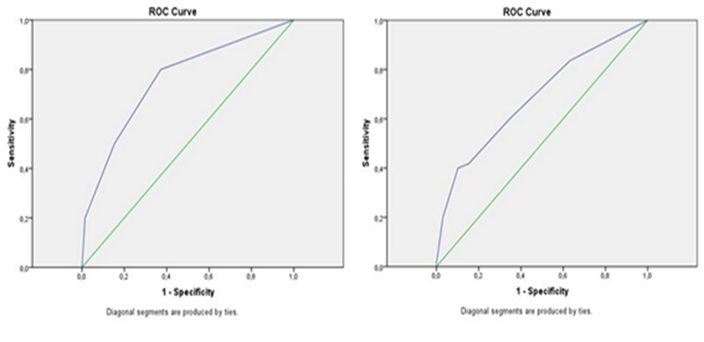
Table 3 describes the multiple logistic regression model for the subtypes of abuse. Only variables that presented p <0.2 in the bivariate analysis were inserted into the model. The area under the Receiver Operating Characteristics (ROC) curve for the logistic regression model was 0.68 (CI 0.59-0.77, p <0.001) for psychological abuse and 0.75 (CI 0.59-0.92, p = 0.007) for physical abuse (Figure 1).
Figure 1 - ROC curve based on the logistic regression model for psychological violence (left image) and physical violence (right image) among elderly residents in the community
A reliability test of the CTS-1 items was performed, analyzing the mean of the item less scale, the item less scale variable, and the Cronbach's alpha (α), where it showed a total score of 0.82.
DISCUSSION
Psychological abuse was the predominant type of abuse in this study. This finding is also present in other cross-sectional study conducted in Brazil, which found a prevalence of 47.4%(16-17). Other studies conducted in the America found a prevalence of 32.4% in Bolivia(12), and 2.7% in Canada(18).
Previous studies have corroborated with the theory of gender as a risk factor for EA occurrence(10,6). A study conducted in Bolivia explained the greater victimization among elderly women was related to patriarchal relations between men and women, in which women are expected to submit to men, thus making women more vulnerable to elder abuse(12).
Findings also indicate that women who experienced emotional abuse prior to age 60 are at greater risk of experiencing abuse after age 60(19). Although the results in our study pointed to a higher prevalence of abuse among women, there was no statistically significant difference between genders.
Data from our study did not find an association between abuse and age, despite other studies findings of higher prevalence of abuse, both psychological and physical, among younger elderly between 60 to 70 years old. These results falls in opposition to others research which suggests that increases in age are related to decreased functional capacity and greater vulnerability to EA(12).
The EA literature identifies that the home environment is the most common place where abuse occurs and is majorly perpetrated by the spouse, adult children, or both(20,17). In the present study, elders who were married or living together were found to have increased probability of suffering abuse, consistent with another Brazilian study that used the CTS-1(8).
Fragile family ties are strong indicators of conflicts that lead to elder abuse. Therefore, a major challenge to EA prevention is to find the balance between the responsibility of the family and the government, both charged with caring for the elderly population, also broadening the access and offer of specialized services, with a focus on minimizing the overburden of the elder immediate caregivers(10).
The importance of family support within the elderly safety net is supported in our study, since elderly without family support presented 3.67 more chances of being victimized than those who reported to have support. This is consistent with multicentric research that showed low family support as a determinant for the occurrence of psychological abuse among elderly people(10).
Our study found increased occurrence of psychological abuse in elderly people with urinary incontinence (UI). A recent study that conceptualized causal and contributing factors among incontinence, care dependence, and elder abuse found that caregivers (formal or family) do not necessarily have knowledge about the etiology of UI or the skills to provide continence care. This may lead to feelings of exhaustion, frustration, disgust or shame(21). These factors coupled with society’s stigmatized view of incontinence and the recipient care characteristics, could cause power struggles resulting in coercion, chastisement, and neglect(21).
The presence of depressive symptoms presented an odds ratio of 4.97 for experiencing physical abuse, corroborating with many other studies that have also shown an association between depression and elder abuse(22). A study that analyzed the influence of elder abuse subtypes in depression found that elder depression is mostly influenced by verbal and emotional abuse rather than by physical abuse, financial exploitation or neglect, opposing the finds of our study in which elders with depressive symptoms had a higher chance of experience physical abuse(23).
The nature of the cross-sectional studies cited above does not allow us to make affirmations about the relationship of cause and effect between depression and elder abuse. It can be also hypothesized that experiencing abuse is what leads to the development of depression. However, it is clear that depression and elder abuse are strongly related, making possible to state that depression can be characterized as both a risk factor for elder abuse and a consequence for victims of EA. Therefore, treating depression figures as an important element to prevent and stop elder abuse(24).
Despite our findings, which found psychological abuse the most prevalent EA subtype, other studies found physical abuse to be the most reported type of abuse(20). The contrasting findings among screening studies in the elderly population and studies that analyze data from reporting systems can be explained by the fact that injury from physical abuse is more easily identified by health professionals, whereas psychological abuse is invisible, leaving no physical marks, but has equally debilitating consequences(9).
A longitudinal study using the CTS-1 scale with British women, concluded that women abused in childhood were four to seven times more likely to suffer from depression when they reached adulthood(25). Although the present study was performed with elderly people and did not use sex as an outcome variable, the results are similar since the elderly female victims of physical abuse presented 4.97 more chances to develop depression than those who were not victims.
Having a paying job was considered as a protection factor for the occurrence of abuse in the elderly women, since it allowed them to find financial autonomy(25). However, for men it was considered a risk factor, since searching for a job may be related to staying away from the conflicting home environment(10). In our study, elders who worked presented an odds ratio of 7.87 for the occurrence of physical abuse in comparison to those who did not work, leading us to conclude that work may be a risk factor for physical abuse among the elderly.
A person assisted by health services will undoubtedly receive care from nursing professionals and if those nurses have forensic training, they may observe injuries and behavioral patterns consistent with EA. Consequently, FN knowledge helps to identify which procedures must be adopted to effectively assist the victim, while at the same time collaborating with the work of justice(25).
We note some limitations of this study. Once EA research is based on self-report, the prevalence of EA might be underestimated since victims may choose to not release all information to the interviewer, either for fear or shame. The cross-sectional design of this study makes it impossible to draw conclusions regarding any causal or temporal relationships between the independent variables and the occurrence of EA.
CONCLUSIONS
Psychological abuse was associated with being married or living together, not have someone to care for the elderly person in case they got sick and suffering urinary incontinence while physical abuse was related to presence of depressive symptoms and having a paying job. Understanding how much these elderly characteristics are able to predict EA can help nurses to intervene more effectively to prevent victimization by targeting these predictors risk factors found in this research.
REFERENCES
1. World Health Organization. Missing voices: Views of older persons on elder abuse. Geneva: World Health Organization; 2002.
2. Schofield MJ, Powers JR, Loxton D. Mortality and disability outcomes of self-reported elder abuse: a 12-year prospective investigation. J Am Geriatr Soc [Internet]. 2013 [citado 2021 Jan 14];61(5):679–85. Doi: https://doi.org/10.1111/jgs.12212
3. Drake SA, Koetting C, Thimsen K, Downing N, Porta C, Hardy P, et al. Forensic nursing state of the science: research and practice opportunities. J Forensic Nurs [Internet]. 2018 [citado 2021 jan. 17];14(1):3-10. Doi: https://doi.org/10.1097/jfn.0000000000000181
4. International Association of Forensic Nursing. History of the IARN. 2019. [citado 2021 Jan 21]. Disponível em: https://www.forensicnurses.org/page/AboutUS
5. Hasselmann MH, Reichenheim ME. Adaptação transcultural da versão em português da Conflict Tactics Scales Form R (CTS-1), usada para aferir violência no casal: equivalências semântica e de mensuração. Cad Saude Publica [Internet]. 2003 [citado 2021 Jan 21];19(4):1083–93. Disponível Doi: https://doi.org/10.1590/S0102-311X2003000400030
6. Gil AP, Santos AJ, Kislaya I, Santos C, Mascoli L, Ferreira AI, et al. A sociography of elderly victims of family violence in Portugal. Cad Saude Publica [Internet]. 2015 [citado 2021 Jan 26];31(6):1234–46. Doi: https://doi.org/10.1590/0102-311X00084614
7. Rodrigues RAP, Monteiro EA, Santos AMR, Pontes MLF, Fhon JRS, Bolina AF, et al. Older adults abuse in three Brazilian cities. Rev Bras Enferm [Internet]. 2017 [citado 2019 Jan 26];70(4):783–91. Doi: http://dx.doi.org/10.1590/0034-7167-2017-0114
8. Santos RC, Menezes RMP de, Gonçalves RG, Silva JC da, Almeida JLS, Araújo GKN. Violence and frailty in the elderly. Rev Enferm UFPE On Line [Internet]. 2018 [citado 2021 Jan 26];12(8):2227–34. Doi: https://doi.org/10.5205/1981-8963-v12i8a234398p2227-2234-2018
9. Guimarães APS, Górios C, Rodrigues CL, Armond JE. Notification of intrafamily violence against elderly women in the city of São Paulo. Rev Bras Geriatr Gerontol [Internet]. 2018 [citado 2021 Jan 30];21(1):88–94. Doi: https://doi.org/10.1590/1981-22562018021.160213
10. Guedes DT, Alvarado BE, Phillips SP, Curcio CL, Zunzunegui MV, Guerra RO. Socioeconomic status, social relations and domestic violence (DV) against elderly people in Canada, Albania, Colombia and Brazil. Arch Gerontol Geriatr [Internet]. 2015 [citado 2021 Jan 30];60(3):492–500. Doi: https://doi.org/https://doi.org/10.1016/j.archger.2015.01.010
12. Carmona-torres JM, López-Soto PJ, Coimbra-roca AI, Gálvez-rioja RM, Goergen T, Rodríguez-Borrego MA. Elder abuse in a developing area in Bolivia. J Interpers Violence [Internet]. 2015 [citado 2021 Fev 03];1–18. Doi: https://doi.org/10.1177/0886260515608803
13. Yan E, Chan K-L, Tiwari A. A systematic review of prevalence and risk factors for elder abuse in Asia. Trauma Violence Abuse [Internet]. 2015 [citado 2021 Fev 03];16(2):199–219. Doi: https://doi.org/http://dx.doi.org/10.1177/1524838014555033
14. Beach SR, Carpenter CR, Rosen T, Sharps P, Gelles R. Screening and detection of elder abuse: Research opportunities and lessons learned from emergency geriatric care, intimate partner violence, and child abuse. J Elder Abuse Negl [Internet]. 2016 [citado 2021 Fev 03];28(4–5):185–216. Doi: https://doi.org/10.1080/08946566.2016.1229241
15. Apóstolo JLA, Loureiro LMJ, Reis IAC, Silva IAL, Cardoso DFB, Sfetcu R. Contribution to the adaptation of the Geriatric Depression Scale -15 into portuguese. Referência [Internet]. 2014 [citado 2021 Fev 03];4(3):65–73. Doi: http://dx.doi.org/10.12707/RIV14033
16. Irigaray TQ, Esteves CS, Pacheco JTB, Grassi-Oliveira R, Argimon IIL. Elder abuse in Porto Alegre, Rio Grande do Sul, Brazil: a documentary study. Estud Psicol [Internet]. 2016 [citado 2021 Fev 04];33(3):543–51. Doi: https://doi.org/10.1590/1982-02752016000300017
17. Garbin CAS, Joaquim RC, Rovida TAS, Garbin AJI. Elderly victims of abuse: A five year document analysis. Rev Bras Geriatr Gerontol [Internet]. 2016 [citado 2021 Fev 11];19(1):87–94. Doi: https://doi.org/dx.doi.org/10.1590/1809-9823.2016.15037
18. McDonald L. The mistreatment of older Canadians: findings from the 2015 national prevalence study. J Elder Abuse Negl [Internet]. 2018 [citado 2021 Fev 15];30(3):176-208. Doi: https://doi.org/10.1080/08946566.2018.1452657
19. Policastro C, Finn MA. Coercive control and physical violence in older adults: analysis using data from the National Elder Mistreatment Study. J Interpers Violence [Internet]. 2015 [citado 2021 Mar 07];32(3):311–30. Doi: https://doi.org/10.1177/0886260515585545
20. Sampaio LS, July MSF, Sampaio TSO, Souza WP, Prado APS, Reis LA. Violência física em idosos. C&D-Rev Elet FAINOR [Internet]. 2017 [citado 2021 Mar 07];10(2):188–200. Disponível em: http://srv02.fainor.com.br/revista/index.php/memorias/article/view/661
21. Ostaszkiewicz J. A conceptual model of the risk of elder abuse posed by incontinence and care dependence. Int J Older People Nurs [Internet]. 2017 [citado 2021 Mar 07];1–11. Doi: https://doi.org/10.1111/opn.12182
22. Rajapakshe OBW, Sivayogan S, Kulatunga PM. Prevalence and correlates of depression among older urban community‐dwelling adults in Sri Lanka. Psychogeriatrics [Internet]. 2019 [citado 2021 Mar 07];19(3):202-11. Doi: https://doi.org/10.1111/psyg.12389
23. Park EO. Most prevalent type of elder abuse and its correlation with elder depression. Acta Paul Enferm [Internet]. 2019 [citado 2021 Mar 07];32(1):95-100. Doi: https://doi.org/10.1590/1982-0194201900013
24. Roepke-Buehler SK, Dong X. Perceived Stress and Elder Abuse: A Population-Based Study of Adult Protective Services Cases in Chicago. Geriatrics [Internet]. 2015 [citado 2021 Mar 12];63(9):1820-28. Doi: https://doi.org/10.1111/jgs.13613
25. Ouellet-Morin I, Fisher HL, York-Smith M, Fincham-Campbell S, Moffitt TE, Arseneault L. Intimate partner violence and new-onset depression: a longitudinal study of women’s childhood and adult histories of abuse. Depress Anxiety [Internet]. 2015 [citado 2021 Mar 12];32(5):316–24. Doi: https://doi.org/10.1002/da.22347
GKNAM: concepção e/ou no planejamento do estudo; obtenção, análise e/ou interpretação dos dados; redação e/ou revisão crítica; e aprovação final da versão publicada.
RQS: concepção e/ou no planejamento do estudo; redação e/ou revisão crítica; e aprovação final da versão publicada.
RSR: obtenção, análise e/ou interpretação dos dados; redação e/ou revisão crítica; e aprovação final da versão publicada.
RCSR: obtenção, análise e/ou interpretação dos dados; redação e/ou revisão crítica; e aprovação final da versão publicada.
ICBSC: redação e/ou revisão crítica; e aprovação final da versão publicada.
ALCG: redação e/ou revisão crítica; e aprovação final da versão publicada.
BMLSB: obtenção, análise e/ou interpretação dos dados; redação e/ou revisão crítica; e aprovação final da versão publicada.
Declaration of conflict of interest
Nothing to declare.
Scientífic editor: Ítalo Arão Pereira Ribeiro. Orcid: https://orcid.org/0000-0003-0778-1447
![]()