REVIEW
ARTICLE
REGISTRATION OF CARE BY THE NURSING
TEAM IN THE PATIENT'S ELECTRONIC MEDICAL RECORD: INTEGRATIVE REVIEW
REGISTRO DE CUIDADOS POR PARTE DEL EQUIPO
DE ENFERMERÍA EN LA HISTORIA CLÍNICA ELECTRÓNICA DEL PACIENTE: REVISIÓN
INTEGRADORA
REGISTRO DA ASSISTÊNCIA PELA EQUIPE DE
ENFERMAGEM NO PRONTUÁRIO ELETRÔNICO DO PACIENTE: REVISÃO INTEGRATIVA
https://doi.org/10.31011/reaid-2025-v.99-n.supl.1-art.2430
Bruna
Stein do Lago Sales1
Kátia
Elaine Aparecida Pereira 2
Jhuliano
Silva Ramos de Souza 3
Roberta
Garcia Gomes4
Roberta
Seron Sanches5
Zélia
Marilda Rodrigues Resck6
1Orcid: https://orcid.org/0009-0006-3848-1673
2Orcid:
https://orcid.org/0009-0001-9842-2302
3Orcid: https://orcid.org/0000-0002-4338-4433
4Orcid: https://orcid.org/0000-0002-0277-4371
5Orcid: https://orcid.org/0000-0001-7557-5560
6Orcid: https://orcid.org/0000-0002-3752-8381
1,2,3,4,5,6 Universidade Federal de Alfenas, Alfenas,
Minas Gerais, Brazil.
Corresponding Author
Jhuliano Silva Ramos de Souza
R. Gabriel Monteiro da Silva, 700 -
Centro, Alfenas - MG, Brazil. CEP: 37130-001. E-mail: jhulianoramoz@hotmail.com
Tel: +55(35)3701-9471.
Submission: 12-11-2024
Approval: 02-04-2025
ABSTRACT
Objective: Identify
scientific evidence on current records and resources used by the nursing team
in the patient's electronic medical record. Methods: This is an
integrative literature review, based on the research question: what is the
current status of nursing care records by the nursing team in the Electronic
Patient Record? Results: Through the database search, 1253 studies were
found, with seven articles ultimately being selected. It was possible to choose
a category entitled “Nursing records of patient care: advantages and
disadvantages in the electronic medical record approach”, with two
subcategories, the first “Advantages of electronic records as tools to
systematize patient care and communication between professionals” and the
second, “Disadvantages and challenges in the use of electronic patient records
in the light of nursing team professionals”. Conclusion: It is pointed
out that nursing records in the patient's electronic medical record allow for
systematization of care, less time for notes and thus more contact time between
nursing team professionals and patients, bringing benefits. However, there are
still difficulties and challenges regarding the use of the tool, which requires
training of the nursing team to optimize the applicability of computerization
for nursing records.
Keywords: Electronic Health Record;
Electronic Patient Record; Nursing Record; Assistance Record; Nursing Team.
RESUMEN
Objetivo: Identificar
evidencia científica sobre registros y recursos actuales utilizados por el
equipo de enfermería en la historia clínica electrónica del paciente. Métodos:
Se trata de una revisión integradora de la literatura, basada en la pregunta de
investigación: ¿cuál es el estado actual de los registros de cuidados de
enfermería por parte del equipo de enfermería en el Registro Electrónico del
Paciente? Resultados: A través de la búsqueda en las bases de datos se
identificaron 1.253 estudios, de los cuales se seleccionaron siete artículos
para el análisis. A partir de esta selección se logró establecer una categoría
denominada “Registro de Enfermería de la Atención al Paciente: Ventajas y
Desventajas de la Historia Clínica Electrónica”. Esta categoría se dividió en
dos subcategorías: la primera, “Ventajas de la Historia Electrónica como
Herramientas para Sistematizar la Atención al Paciente y la Comunicación entre
Profesionales”; y el segundo, “Desventajas y desafíos en el uso de registros
electrónicos de pacientes desde la perspectiva del equipo de enfermería”. Conclusión:
Se destaca que los registros de enfermería en la historia clínica electrónica
del paciente permiten la sistematización de los cuidados, menor tiempo para
notas y, por tanto, mayor tiempo de contacto entre los profesionales del equipo
de enfermería y los pacientes, trayendo beneficios. Sin embargo, aún existen
dificultades y desafíos en cuanto al uso de la herramienta, lo que requiere la
capacitación del equipo de enfermería para optimizar la aplicabilidad de la
informatización de los registros de enfermería.
Palabras
clave:
Historia clínica electrónica; Historial Electrónico del Paciente; Registro de Enfermería;
Registro de Asistencia; Equipo de Enfermería.
RESUMO
Objetivo: Identificar as
evidências científicas sobre os registros e recursos atuais utilizados pela
equipe de enfermagem no prontuário eletrônico do paciente. Métodos:
Trata-se de uma revisão integrativa da literatura, baseada na questão da
pesquisa: qual a situação atual dos registros da assistência de enfermagem pela
equipe de enfermagem no Prontuário Eletrônico do Paciente? Resultados: Por
meio da busca na base de dados, foram identificados 1.253 estudos, dos quais
sete artigos foram selecionados para análise. A partir dessa seleção, foi
possível estabelecer uma categoria intitulada “Registro de Enfermagem da
Assistência aos Pacientes: Vantagens e Desvantagens do Prontuário Eletrônico”.
Esta categoria foi dividida em duas subcategorias: a primeira, “Vantagens dos
Registros Eletrônicos como Ferramentas para Sistematizar o Cuidado ao Paciente
e a Comunicação entre Profissionais”; e a segunda, “Desvantagens e Desafios no
Uso do Prontuário Eletrônico do Paciente sob a Perspectiva da Equipe de
Enfermagem”. Conclusão: Aponta-se que os registros de enfermagem no
prontuário eletrônico do paciente permitem sistematizar o cuidado, menor tempo
para as anotações e assim, maior tempo de contato dos profissionais da equipe
de enfermagem com os pacientes, trazendo benefícios. No entanto, ainda há
dificuldades e desafios presentes quanto ao uso da ferramenta, o que requer a
capacitação da equipe de enfermagem para otimizar a aplicabilidade da
informatização para os registros de enfermagem.
Palavras-chave: Registro Eletrônico de Saúde; Prontuário
Eletrônico do Paciente; Registro de Enfermagem; Registro da Assistência; Equipe
de Enfermagem.
INTRODUCTION
Nursing records
are a vital form of written communication that contains crucial information
about the patient and the care provided by the nursing team, assisting in the
preparation of the care plan, providing support for the evaluation of care,
monitoring the patient's progress, facilitating nursing audits and contributing
to teaching and research in the area (1).
In 2012, the
Federal Nursing Council (COFEN) established that it is the responsibility and
duty of nursing team professionals to record, in the patient's medical records
and other specific documents, information inherent to the care process and the
management of work processes (2).
To this end,
nursing notes are a means of communication between the teams that participate
in the comprehensive treatment of patients, in addition to being important care
and epidemiological indicators, thus used in statistics (1).
It is worth noting
that electronic medical records assist in prevention, diagnosis, treatment,
health recovery, and provide data for indicators. Furthermore, electronic
records provide information and legal evidence to medical institutions and
pharmaceutical companies (3).
Nursing produces
a lot of information related to patient care on a daily basis, and it is
estimated that it is responsible for more than 50% of the information contained
in patient records. Therefore, there is an undeniable need for adequate and
frequent records in the medical record (4).
In 2024, the
Federal Nursing Council will align the computerized information system and
standardize the use of electronic medical records and digital platforms in the
nursing field, making it the responsibility and duty of nursing professionals
to record, in the patient's medical record, the information related to the care
process and the management of work processes, in order to allow continuity of
care (5).
It is recommended
that the medical records include data related to the patient identification
protocol, such as full name and date of birth, medical history, treatment plan,
reports of complementary exams, medical prescription and nursing progress,
consent forms, reasons for transfer, discharge or death and various documents (6).
It is important to
emphasize that the lack of information related to the care provided to patients
and the absence of a standard in the descriptions of clinical conditions and
patient progress hinder communication between multidisciplinary health teams
and have a negative impact on the quality of care (1). In addition,
a properly completed medical record, in a technical and organized manner, can
serve as a legal basis to refute allegations of malpractice, recklessness or
negligence (7-8).
It confirms that
this instrument can be used as a legal document to defend or incriminate
professionals in various legal spheres, since, having performed the procedures
safely and within technical, ethical and legal principles, the nursing
professional is protected in cases of doubts or future questions (9).
From this
perspective, it evolved into a computerized information system that provides
all members of the nursing team with the data necessary for the development of
care, as well as optimizing the communication process between the members of
the multidisciplinary team and the client (10).
In this context,
the objective of this work is to identify scientific evidence on the current
records and resources used by the nursing team in the patient's electronic
medical record.
METHODS
This
is an integrative literature review that allows us to understand a specific
issue or event, while contributing to evidence-based practice through relevant
studies that support decision-making and identify gaps for new research (11).
The
research protocol was registered in May 2024 by the Fighsare repository
(https://figshare.com), following the methodological framework (11),
in which the respective Digital Object Identifier (DOI) was generated:
10.6084/m9.figshare.25748946.
Data
collection was performed through six steps described in the literature: I)
elaboration of the guiding question; II) search or sampling in the literature;
III) data collection; IV) critical analysis of the included studies; V)
discussion of the results and VI) presentation of the integrative review (11).
The
research question was defined using the PICo strategy (acronym for
Patient-Intervention-Context)(12) to describe the following
elements: P (population/problem): Nursing Team, I (intervention): Nursing care
records; Co (context): Electronic Patient Record. This research aims to answer
the following question: What scientific evidence is available on the current
status of nursing records by the team in the Electronic Patient Record?
The
Virtual Health Library (VHL) was used as the database for searching for primary
studies: LILACS (Latin American and Caribbean Literature in Health Sciences),
PUBMED (National Library of Medicine), SCIELO (Scientific Electronic Library
Online), Web of Science (WOS) and SCOPUS (Elsevier).
The
search was conducted using controlled and uncontrolled descriptors and
combinations with the Boolean operators “AND”, “OR”: Electronic Health Record
OR Electronic Nursing Record; Nursing Record OR Care Record; “AND” Nursing
Team.
Full
primary articles in Portuguese, English and Spanish, published in the last ten
years, available free of charge online, were included. Studies from gray
literature such as books, theses, dissertations, monographs, abstracts,
editorials, and reviews were excluded.
Data
collection took place in March and April 2024, and was carried out blindly by
two independent researchers. Throughout the searches in the databases, the
collected articles were exported to the EndNote x9 reference manager, online
version, for the inclusion and exclusion criteria mentioned above. The search
was guided by the crossing of the elements of the PICo strategy.
The
Rayyan Systems Inc. web application was also used, which assists researchers in
selecting studies in review methods. It is an agile and effective tool,
according to the blinding performed by the researchers (13). The
collected data were reread by the third researcher, the advisor.
Immediately
after using the tools, the information was aligned in order to highlight the
title, author, year, methodology, results and conclusion.
The
criterion for analyzing the levels of evidence was the classification into
seven levels, namely: level 1 - systematic review or meta-analysis of a
randomized controlled clinical trial; level 2 - randomized controlled clinical
trial; level 3 - controlled clinical trial without randomization; level 4 -
case control or cohort; level 5 - systematic review of qualitative and
descriptive studies; level 6 - qualitative and descriptive studies; level 7 -
opinion (14).
Next,
the data were interpreted and categorized in a succinct and methodological
manner for this
integrative review presents a total of 1,253 articles found in the databases
(Lilacs=104; themes related to the objective of the study, for discussion.
RESULTS
Pubmed=10;
Scielo=98; Scopus=319; Web of Science=722). Of this total, 244 duplicates were
excluded. After reading the title and abstract, eight articles remained, which
were selected for full reading. After reading, one article was excluded because
it was monetized. The final sample consisted of seven articles, which were
included in this review (Figure 1).
Figure 1
- Flowchart for selecting primary studies. Alfenas, Minas Gerais, 2024.
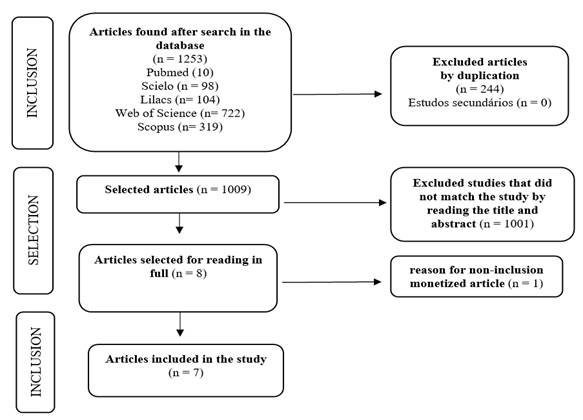
Table 2 summarizes the main
evidence from the seven selected studies, including information on study
titles, authors, year of publication, journal, objective, type of study, main
results and level of evidence. Regarding the years of publication, only two
studies were published in the last 5 years and the others are from previous
years.
DISCUSSION
The
articles selected in this integrative literature review indicate that, in the
current situation, nursing care records are concentrated in the Electronic
Patient Record. For the discussion, a main category was identified, subdivided
into two subcategories.
Nursing records of
patient care: advantages and disadvantages of the electronic medical record
approach
This
is the only category in which the Electronic Patient Record (EPR) is presented
as an essential tool for recording health and disease data, indispensable for
communication between the multidisciplinary team and the patient (15).
Considering
that the nursing team is responsible for most of the records in the patient's
medical record, these must always be updated and regulated so that they are
effective in their function of demonstrating the care provided and reflecting,
objectively, the application of each of the stages of the Nursing Process (16).
It
is shown that nursing professionals indicate advantages and disadvantages in
relation to the EPR, constituting the two subcategories.
Advantages of electronic
records as tools to systematize patient care and communication between
professionals
In
this subcategory, it is shown that in the usability assessment, the EHR
presented positive points regarding suitability for the task, in accordance
with the user's expectations and tolerance to error. And, it is also related to
the use, satisfaction and acceptance of the system, as well as the time
required to record the data (15).
In
addition, it has the capacity to store all of the patient's health,
administrative and clinical information, in contrast to the conventional
medical record. The security offered by the use of an electronic record is
observed when the EHR allows for backups to be made, to avoid loss of
information, and the legality of the records, in relation to the physical
medical record, since the typed record allows for greater understanding (17).
Concerning
the use of the EHR by nurses and nursing technicians, it is noted that it is
easy to use, since people with better computer skills can handle technological
tools more easily. Furthermore, it was identified that the operating system
used facilitates recall, manipulation and access, which favors the fact that a
small portion of the population studied reported having difficulty in
understanding or handling the EHR (17).
It
is also noted that electronic records enable more efficient interdisciplinary
collaboration through the availability of data and synthesis of information, as
well as improving patient safety, since the use of the EHR is an efficient way
to clarify, document and communicate basic care elements to the health team, in
addition to organizing and guiding nurses' thinking and clinical
decision-making (18).
It
is also noted that the electronic health record has been described as a factor
that facilitates teamwork in primary care, capable of improving communication
within the team through better access to information, as well as facilitating
the redefinition of tasks and team functions (19).
Another
advantage of electronic records is that by applying a systematic approach, a
set of essential clinical data on patient admission, recorded on other forms
required for admission, can be brought together in a single electronic form,
making it easier for nursing staff to complete admission documentation (20).
Disadvantages and
challenges in using electronic patient records in light of nursing team
professionals
One
disadvantage and challenge that institutions must face is that the EHR is part
of the daily routine of health services and many nurses and nursing technicians
still do not feel confident in using it, requiring assistance to access basic
commands (15).
It
is attributed that the need for help to work with information resources came
from the lack of training and qualification of professionals (17). It is also worth noting that if
professionals are not trained, communication failures may occur between members
of the multidisciplinary health team, which may impair patient care. Therefore,
for the EHR to be an effective technological tool, it must be the object of
training, facilitating the qualification of professionals (15).
It
is therefore emphasized that there is a close relationship between training and
the use of the EHR and its use without difficulties by health professionals (17). It is also corroborated as a disadvantage
of the EHR, the system failures, that is, when the system becomes inoperative.
These failures end up compromising access to patients' electronic documents
and, consequently, quality care. To this end, there is a need for greater
investment in systems, equipment and software, which are essential to ensure
that failures become less frequent (17).
It
is argued that excessive documentation and information in electronic records
does not add value to the healthcare team's processes. It is considered that
optimizing the choice of content for items and information that make up the EHR
and presenting them in a way that best supports decision-making processes is an
issue that is still not well understood, which becomes a disadvantage in the
use of the EHR (20-21).
Healthcare
professionals report spending time reviewing information in electronic records
and only a few specific areas are frequently reviewed, which contain important
data for patient care. Many areas of the EHR are rarely accessed for review,
requiring the reformulation of electronic records in order to streamline and
reduce complexities and redundancies in documentation (22).
Professionals
noted that the form was also perceived as inflexible, as it did not allow the
user to access other sections of the electronic record while it was open and
after it was started. Repetition of information and duplication of tasks were
frequently cited as challenges (20).
To
this end, many electronic health records require improvements in their
functionality to support teamwork, particularly with regard to comprehensive
care plans and longitudinal tracking of patient data (19).
CONCLUSIONS
It
was possible to consider that currently, most records are being made in a computerized
manner, through the use of the EHR, allowing the systematization of care,
reducing the time spent on documenting patient information, eliminating
redundancies, improving communication time between the team, optimizing access
to information and providing information to the multidisciplinary team. It is
pointed out that the facilitators of the use of the EHR converge to increase
contact between the care team and the patient, which is fundamental for
comprehensive care and patient safety.
This
integrative review was limited by the few studies found on the topic addressed,
thus limiting the understanding of the current situation of nursing records in
a broad way. It is inferred that there is a need for scientific productions
aiming at greater scientific evidence, since this review identified articles
with level four and five evidence.
It
is expected that this study will contribute to the training of future nursing
professionals and in their qualification regarding the importance of nursing
records and the use of the EHR. Furthermore, it is expected to reach
professionals working in clinical nursing practice so that the challenges
regarding the use of electronic records can be overcome.
The
evidence from this study has implications for nursing services, nursing
education and administration, as well as in the scientific context, since it
brings relevant contributions to future research. However, it is worth
highlighting that all these advantages are not achievable if nursing team
professionals do not receive constant training and qualifications to equip them
with the tools to use the EHR and master the computerization of nursing
records.
REFERENCES
1.
Omizzolo JE, Ramos KS. Registros de enfermagem: um instrumento para a qualidade
da assistência. Inova Saúde [Internet]. 2021 [acesso 2024 Abr 12];11(1):1-16. Disponível em:
https://periodicos.unesc.net/ojs/index.php/Inovasaude/article/view/5254/5622.
2.
Conselho Federal de Enfermagem (BR). Resolução COFEN Nº 429/2012. Dispõe sobre
o registro das ações profissionais no prontuário do paciente, e em outros
documentos próprios da enfermagem, independente do meio de suporte -
tradicional ou eletrônico [Internet]. Brasília: DF: COFEN; 2012 [acesso 10 jan
2024]. Disponível
em: https://www.cofen.gov.br/resoluo-cofen-n-4292012/
3. Sun J, Yao X, Wang S, Wu Y. Blockchain-based
secure storage and access scheme for electronic medical records in ipfs. IEEE Access
[Internet]. 2020 [acesso 2024 Abr 12];8:59389-401. Disponível em:
http://dx.doi.org/10.1109/access.2020.2982964.
4.
Ferreira LL, Chiavone FBT, Bezerril MS, Alves KYA, Salvador PTCO, Santos VEP.
Análise dos registros de técnicos de enfermagem e enfermeiros em prontuários.
Rev Bras Enferm [Internet]. 2020 [acesso 2024 Abr 12]; 73(2):e20180542.
Disponível em: https://doi.org/10.1590/0034-7167-2018-0542
5.
Conselho Federal de Enfermagem (BR). Resolução COFEN nº754 de 16 de maio de
2024. Normatiza o uso do prontuário eletrônico e plataformas digitais no âmbito
da Enfermagem: digitalização, utilização de sistemas informatizados para guarda
e armazenamento nesta tecnologia. [Internet]. Brasília: DF: COFEN; 2024. [acesso
2024 Jan 10]. Disponível
em: https://www.cofen.gov.br/?p=128256&preview=true.
6.
Conselho Federal de Enfermagem (BR). Resolução COFEN nº 358/2009. Dispõe sobre
a Sistematização da Assistência de Enfermagem e implementação do Processo de
Enfermagem em ambientes, públicos ou privados, em que ocorre o cuidado
profissional de Enfermagem, e dá outras providências [Internet]. Brasília: DF:
COFEN; 2009 [acesso 2024 Jan 10]. Disponível em:
https://www.cofen.gov.br/resoluo-cofen-3582009/
7.
Conselho Federal de Enfermagem (BR). Resolução COFEN nº 564/2017. Aprova novo
Código de Ética dos Profissionais de Enfermagem. [Internet]. Brasília: DF:
COFEN; 2017. [acesso 2024 Jan 10]. Disponível em:
http://www.cofen.gov.br/resolucao-cofen-no-5642017_59145.html.
8.
Brasil. Lei nº 10.406, de 10 de janeiro de 2002. Institui o Código Civil
[Internet]. Brasília: DF; 2002 [acesso 2024 Jan 10]. Disponível em: https://www2.camara.leg.br/legin/fed/lei/2002/lei-10406-10-janeiro-2002-432893-publicacaooriginal-1-pl.html
9.
Conselho Regional de Enfermagem de Santa Catarina (BR). Legislação comentada:
lei do exercício profissional e código de ética. v. 3 [Internet]. Florianopolis:
SC: Coren-SC; 2016;
140 p. [acesso
2024 Jan 10].
Disponível
em:
http://www.corensc.gov.br/wp-ontent/uploads/2016/11/Legisla%C3%A7%C3%A3o-Comentada_site.pdf.
10.
Oliveira AF de S, Lopes Junior HMP, Silva LG da. Impacto da auditoria de
enfermagem na gestão de recursos e custos em instituições de saúde. REASE
[Internet]. 2024 [acesso 2024 Nov 12];10(10):26-38. Disponível em: https://doi.org/10.51891/rease.v10i10.15835
11.
Souza MT, Silva MD, Carvalho R. Revisão integrativa: o que é e como fazer. Revista
Einstein [Internet] 2010 [acesso 2024 Nov 12]8(1):102-6. Disponível em:
http://www.scielo.br/pdf/eins/v8n1/pt_1679-4508-eins-8-1-0102.pdf.
12.
Araújo W, Oliveira C. Recuperação da informação em saúde: construção, modelos e
estratégias. Conv. Ciênc. Inform [Internet] 2020 [acesso 2024 Maio
23]3(2):100-34. Disponível em:
https://doi.org/10.33467/conci.v3i2.13447.
13. Ouzzani M, Hammady H, Fedorowicz Z,
Elmagarmid A. Rayyan-a web and mobile app for systematic reviews. Systematic
Reviews [Internet] 2016 [acesso
2024 Nov 12];5(210). Disponível
em:
https://doi.org/10.1186/s13643-016-0384-4
14.
Fineout-Overholt E, Stillwell SB. Asking compelling, clinical
questions. In Evidence-Based Practice in Nursing & Healthcare: A Guide to
Best Practice (Melnyk BM & Fineout-Overholt E eds). Wolters Kluwer,
Lippincott Williams & Wilkins; 2011 [acesso 2024 Nov 12]; 2:25-39.
15. Lahm JV, Carvalho DR. Prontuário
eletrônico do paciente: avaliação de usabilidade pela equipe de enfermagem. Cogitare
Enferm.
[Internet] 2015 [acesso
2024 Nov 12]; 20(1):1-11. Disponível em:
http://dx.doi.org/10.5380/ce.v20i1.36485. 13
16.
López-Cocotle JJ, Moreno-Monsiváis MG, Saavedra-Vélez CH. Construcción y
validación de un registro clínico para la atención asistencial de enfermería. Enferm.
Universitaria [Internet]
2017. [acesso
2024 Nov 12]14(4):293-30. Disponível em:
http://dx.doi.org/10.1016/j.reu.2017.08.00
17.
Barros MMO, Damasceno CKCS, Coelho MCVS, Magalhães JM. Utilização do prontuário
eletrônico do paciente pela equipe de enfermagem. Rev. enferm. UFPE
on line [Internet] 2020. [acesso
2024 Nov 12] Disponível
em:
http://dx.doi.org/10.5205/1981-8963.2020.241496.
18. Englebright J, Aldricj K, Taylor CR. Defining
and incorporating basic nursing care actions into the electronic health record.
J. Nurs. Scholarsh. [Internet] 2014 [acesso 2024 Nov 12];46(1):50-7. Disponível
em: http://dx.doi.org/10.1111/jnu.12057
19.
O’Malley AS, Draper K, Cross DA, Scholle AH. Electronic health
records and support for primary care teamwork. JAMIA Open. [Internet] 2015 [acesso
2024 Maio 20];22(2):426-34. Disponível em:
http://dx.doi.org/10.1093/jamia/ocu029
20. Shala DR, Jones A, Fairbrothe G, Davis
J, Macgregor A, Baysari M. Adopting an American framework to optimize nursing
admission Documentation in an Australian health organization. JAMIA Open.
[Internet] 2022 [acesso
2024 Maio 20];11;5(3):ooac054. Disponível em:
https://doi.org/10.1093/jamiaopen/ooac054.
21. Pickering BW, Gajic O, Ahmed A,
Herasevich V, Keegan MT. Data utilization for medical decision making at the
time of patient admission to ICU. Crit Care Med [Internet]. 2013. [acesso 2024
Maio 20];1(6):1502-10. Disponível em:
https://doi.org/10.1097/CCM.0b013e318287f0c0.
22. Penoyer DA, Cortelyou-Ward KH, Noblin
AM, Bullard T, Talbert S, Wilson J, Schafhauser B, Briscoe JG, et al. Use of
electronic health record documentation by healthcare workers in an acute care
hospital system. J
Healthc Manag [Internet] 2014[acesso 2024 Maio 20];59(2):130-44. Disponível em:
https://journals.lww.com/jhmonline/abstract/2014/03000/use_of_electronic_health_record_documentation_by.8.aspx
No
funding
Authorship
criteria (authors' contributions)
1.
contributed substantially to the design and/or planning of the study: Sales
BSL, Pereira KEAP.
2.
in obtaining, analyzing, and/or interpreting the data: Sales BSL, Pereira KEAP,
Souza JSR, Resck ZMR.
3.
as well as in the writing and/or critical review and final approval of the
published version: Sales BSL, Pereira KEAP, Gomes, RG, Sanches, RS, Souza JSR,
Resck ZMR.
Declaration
of conflict of interests
The
manuscript is extracted from the final course work “Recording of care by the
nursing team in the patient's medical record: integrative literature review”,
defended in 2024, in the Undergraduate Course in Nursing, at the Federal
University of Alfenas.
Scientific Editor: Ítalo Arão
Pereira Ribeiro. Orcid: https://orcid.org/0000-0003-0778-1447
Rev Enferm Atual In Derme
2025;99(supl.1): e025055