REVIEW ARTICLE
RISK FACTORS FOR MATERNAL NEAR MISS: AN INTEGRATIVE LITERATURE REVIEW
FACTORES DE RIESGO PARA EL NEAR MISS MATERNO: UNA REVISIÓN INTEGRATIVA DE LA LITERATURA
FATORES DE RISCO PARA NEAR MISS MATERNO: UMA REVISÃO INTEGRATIVA DA LITERATURA
https://doi.org/10.31011/reaid-2026-v.100-n.1-art.2672
1Jeane Araújo Costa
2Natália Pereira Marinelli
3Layana Pachêco de Araújo Albuquerque
4Kélvya Fernanda Almeida Lago Lopes
1Universidade Federal do Piauí (UFPI), Teresina, Brazil. Orcid: https://orcid.org/0009-0003-3610-6325
2Universidade Federal do Piauí (UFPI), Teresina, Brazil. Orcid: https://orcid.org/0000-0003-4696-3518
3Universidade Federal do Piauí (UFPI), Teresina, Brazil. Orcid: https://orcid.org/0000-0001-6476-4809
4Universidade Estadual do Maranhão (UEMA), Caxias, Brazil. Orcid: https://orcid.org/0000-0002-6320-3492
Corresponding Author
Jeane Araújo Costa
Rua 15 de Novembro, 554, Bairro São José, 64.218.230, Parnaíba – PI. Brazil. E-mail: je.a.costaphb@gmail.com
Submission: 06-10-2025
Approval: 15-01-2026
ABSTRACT
Objective: To identify in the literature the risk factors for Maternal Near Miss (MNM). Methods: This is an integrative review conducted in the Scopus, Embase, LILACS, and BDENF databases, including primary studies published in Portuguese, English, or Spanish. The selection process followed predefined inclusion and exclusion criteria, considering samples of pregnant and postpartum women with records of severe complications during pregnancy, childbirth, or the puerperium. Results: A total of 21 studies from different countries, such as Brazil, Ethiopia, India, and China, were included, revealing a wide diversity of contexts and healthcare realities. The main risk factors associated with MNM were chronic and gestational hypertension, postpartum hemorrhage, anemia, history of cesarean section, inadequate prenatal care, residence in rural areas, and low educational level. Other factors, such as advanced maternal age and unfavorable socioeconomic conditions, were also relevant. Conclusion: Multiple clinical and sociodemographic factors are associated with MNM, highlighting the importance of early detection, continuous monitoring, and qualified prenatal care to reduce severe maternal morbidity.
Keywords: Content Validation; Maternal Near Miss; Obstetrics; Tracking Tools; Validation Study.
RESUMO
Objetivo: Identificar na literatura os fatores de risco para Near Miss Materno (NMM). Métodos: Trata-se de uma revisão integrativa realizada nas bases de dados Scopus, Embase, LILACS e BDENF, contemplando estudos primários publicados em português, inglês ou espanhol. A seleção foi conduzida com base em critérios de inclusão e exclusão previamente definidos, considerando amostras de gestantes e puérperas com registro de complicações graves durante a gestação, parto ou puerpério. Resultados: Foram incluídos 21 estudos provenientes de diferentes países, como Brasil, Etiópia, Índia e China, evidenciando ampla diversidade de contextos e realidades assistenciais. Os principais fatores de risco associados ao NMM foram hipertensão crônica e gestacional, hemorragia pós-parto, anemia, histórico de cesariana, inadequação do pré-natal, residência em áreas rurais e baixa escolaridade. Outros fatores, como idade materna avançada e condições socioeconômicas desfavoráveis, também apresentaram relevância. Conclusão: Conclui-se que múltiplos fatores clínicos e sociodemográficos estão associados ao NMM, reforçando a importância da detecção precoce, do acompanhamento contínuo e da qualificação da atenção pré-natal para a redução da morbidade materna grave.
Palavras-chave: Estudo de Validação; Near Miss; Ferramentas de Rastreamento; Obstetrícia; Validação de Conteúdo.
RESUMEN
Objetivo: Identificar en la literatura los factores de riesgo para el Near Miss Materno (NMM). Métodos: Se trata de una revisión integrativa realizada en las bases de datos Scopus, Embase, LILACS y BDENF, que incluyó estudios primarios publicados en portugués, inglés o español. La selección se llevó a cabo con base en criterios de inclusión y exclusión previamente definidos, considerando muestras de gestantes y puérperas con registro de complicaciones graves durante el embarazo, el parto o el puerperio. Resultados: Se incluyeron 21 estudios provenientes de diversos países, como Brasil, Etiopía, India y China, que evidenciaron una amplia diversidad de contextos y realidades asistenciales. Los principales factores de riesgo asociados al NMM fueron hipertensión crónica y gestacional, hemorragia posparto, anemia, antecedente de cesárea, atención prenatal inadecuada, residencia en áreas rurales y bajo nivel educativo. Otros factores, como la edad materna avanzada y las condiciones socioeconómicas desfavorables, también fueron relevantes. Conclusión: Existen múltiples factores clínicos y sociodemográficos asociados al NMM, lo que resalta la importancia de la detección precoz, el seguimiento continuo y la atención prenatal calificada para reducir la morbilidad materna grave.
Palabras clave: Estudio de Validación; Casi Muerte Materna; Herramientas de Seguimiento; Obstetricia; Validación de Contenido.
INTRODUCTION
The maternal mortality ratio is an important indicator for assessing the presence of inequities in the determinants of health in a given region. Therefore, high maternal mortality ratios suggest the existence of shortcomings in women's healthcare during the pregnancy and postpartum period.
In view of this, in 1990, through the Millennium Development Goals, global targets were established for reducing maternal mortality to 35 deaths per 100,000 live births by 2015. With the end of that year's agenda, a new global target was agreed upon for 2030, based on the Sustainable Development Goals, which set the target at less than 30 maternal deaths per 100,000 live births, so that no country has a maternal mortality rate that exceeds twice the global average.(1)
However, discrepancies are observed in the achievement of the target among nations: the WHO report of 2020 counted 287,000 maternal deaths, with rates of 430 deaths per 100,000 live births in low-income countries and 12 in high-income countries, highlighting the impact of disparities. socioeconomic factors and the higher risk of maternal mortality in vulnerable contexts, generally associated with difficulties in timely access to obstetric care during prenatal care, childbirth, or the postpartum period.(2)
Although maternal mortality is a relevant indicator, the analysis of severe maternal morbidity, such as Maternal Near Miss (MMN), is essential because it presents a higher incidence and similar predictive factors, allowing the identification of failures in maternal health care. According to the WHO, Maternal Near Miss is defined as "a woman who nearly died but survived a complication that occurred during pregnancy, childbirth, or up to 42 days after the end of gestation". (2-3) To create an indicator capable of analyzing severe maternal complications, the WHO standardized criteria for identifying cases of MNM.
The classification of MNM can be done through three approaches: clinical criteria, related to specific diseases (such as pre-eclampsia and its complications, for example, renal failure); Intervention-based criteria, when the pregnant or postpartum woman undergoes procedures such as ICU admission, cesarean section, or blood transfusion; and organ system dysfunction criteria, applicable in the face of sequences of physiological dysfunctions with a risk of death.(3)
In this way, the use of a classification system has enabled a better understanding of the obstacles and solutions in NMM, assisting in the identification of failures in obstetric care and in the reduction of complications and maternal mortality. Investigating risk factors for NMM allows for the evaluation of obstetric services and the implementation of more targeted policies. Thus, this study aimed to identify risk factors for NMM in pregnant or postpartum women in different healthcare settings, such as hospitals and maternity wards.
METHODS
This is an integrative literature review that sought to understand the risk factors for NMM in the context of hospitals and maternity wards. This research method consists of the systematic and structured compilation, evaluation, and synthesis of evidence from the scientific literature in order to develop conclusions about a specific topic.
The development of this study took place in six stages: elaboration of the guiding research question; definition of inclusion and exclusion criteria; choice of descriptors and search strategy; investigation in databases and selection of articles; full reading and critical evaluation of the included evidence; and discussion of the results.
Firstly, to elaborate the guiding research question, the domains of the PICo strategy were used, where Population (P) refers to pregnant women or those in the immediate postpartum period; Phenomenon of Interest (I) to risk factors for NMM; and Context (Co) to hospitals and maternity wards. Thus, this study was guided by the following question: “What are the risk factors for maternal near miss among pregnant women or in the immediate postpartum period in different healthcare settings, such as hospitals and maternity wards?”
Consequently, in the second stage, inclusion and exclusion criteria were defined for manuscript selection. Therefore, primary studies in English, Portuguese, or Spanish, available in full text and answering the guiding research question, were included. Regarding exclusion criteria, review studies, editorials, duplicate articles, and those that did not meet the inclusion criteria were deleted from the research.
The bibliographic survey was conducted in August and September 2024, through access to the Scopus, Embase, Latin American and Caribbean Literature in Health Sciences (LILACS), and Nursing Database (BDENF) databases via the Virtual Health Library (VHL). For the search, controlled and uncontrolled descriptors were chosen after consulting the Health Sciences Descriptors (DeCS) and Medical Subject Headings (MeSH). The combination was performed using the Boolean operators AND and OR.
The descriptors in Portuguese and English selected from DeCS and MeSH were, respectively: Pregnancy; Pregnant Women; "Postpartum Period"; Puerperal Women; "Severe Maternal Complications"; "Risk Factors"; "Maternal Mortality"; Hospital; "Hospitals, Maternity"; "Ambulatory Care Facilities" and "Pregnant Women"; "gravid"; "estates"; "Postpartum Period"; "postpartum periodont"; "puerperal"; "Near miss, Healthcare"; "Near miss Maternal"; "Risk Factors"; "Maternal Mortality"; "Hospitals"; "Hospitals, Maternity"; "Ambulatory Care Facilities"
Initially, the search yielded 64 manuscripts, of which 7 were from the Scopus database, 17 from BVS, and 40 from Embase. After applying the inclusion and exclusion criteria, the final sample consisted of 21 articles.
Figure 1 - Adapted PRISMA flowchart for selecting articles included in the integrative literature review. Teresina, Piauí, Brazil. 2025.
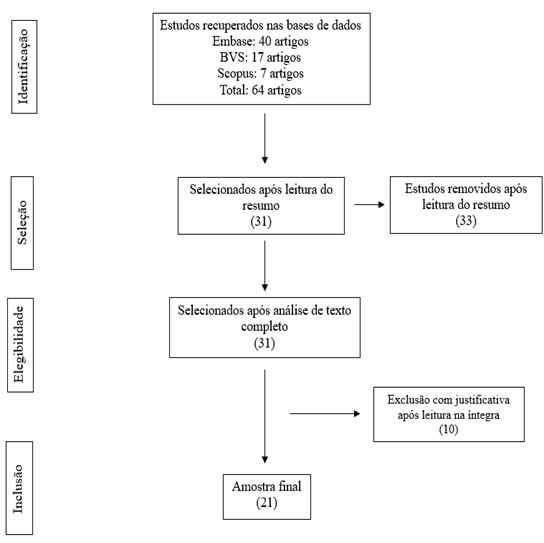
Source: authors (2025).
RESULTS
Of the 21 articles included, six were conducted in Ethiopia, six in Brazil, three in India, two in China, and one each in Cuba, Uruguay, Africa, and Iran, highlighting the geographical diversity of the sample and allowing for the analysis of NMM under different realities. Regarding the year of publication, there were four articles from 2016; three from 2020, 2019, and 2018; two from 2022; and one each from 2023, 2021, 2017, 2015, 2014, and 2011. The absence of a temporal delimitation allowed for the inclusion of a larger number of manuscripts, expanding the volume of results analyzed.
Thus, based on a full reading of the 21 manuscripts, the sample was characterized according to authorship, article title and study location, year of publication, and main results.
Chart 1 - Characterization of the studies included in the review according to authors, title, year, location, and main results. Teresina, Piauí, Brazil, 2025.
|
AUTHOR |
TITLE |
YEAR |
COUNTRY |
MAIN RESULTS AND CONCLUSIONS |
|
Chhavi, Suri, Bachani, Bharti, Pratima Mittal, (4)
|
Carle’s obstetric early warning score as a screening tool for criticacal care admission |
2023 |
India |
Despite progress, maternal mortality remains high in developing countries, affecting families and communities. |
|
Teshome, Ayele, Hailemeskel, Yimer, Mulu, Tadese, (5) |
Determinants of maternal near-miss among women admitted to public hospitals in North Shewa Zone, Ethiopia: A case-control study |
2022 |
Ethiopia |
A history of cesarean section and chronic diseases increase the risk of serious maternal complications and MNM; screening for non-communicable conditions during prenatal care can reduce these events. |
|
Andrade, Bonifácio, Sanchez, Ciabati, Zaratini, (6)
|
Factors associated with serious maternal morbidity in Ribeirão Preto, São Paulo State, Brazil: a cross-sectional cohort study |
2022 |
Brazil |
Trends from 2000 to 2014 show an increase in maternal near misses in the North and Northeast regions of Brazil and a reduction in the South and Southeast regions; severe morbidity associated with risk groups highlights the need for continuous obstetric assessment during prenatal care. |
|
Tenaw, Assefa. Teshale Mulatu, Tura, (7)
|
Maternal near miss among women admitted in major private hospitals in astern Ethiopia: a retrospective study |
2021 |
Ethiopia |
Anemia and chronic hypertension increase the risk of MNM; iron supplementation and nutritional intervention during pregnancy can reduce this risk. |
|
Luna, Rúa, Ordoñez, Fernández, Vidarte, (8)
|
Description of criteria for near miss in high-complexity obstetric population with sickle cell anemia: an observational study |
2020 |
Brazil |
Elevated near miss in pregnant women with sickle cell trait (Hb AS); multidisciplinary follow-up is recommended. |
|
Krishna Kumar, Joshi, Saraswat, Jose, Kapoor, Saha, (9)
|
Near‐Miss Incidents in Obstetric Patients Admitted to an Intensive Care Unit of a Tertiary Care Center in Eastern India: A Retrospective Cohort Study |
2020 |
India |
Pre- and postpartum risk factors, such as severe pre-eclampsia, hemorrhage, hypothyroidism, and diabetes, increase ICU admissions; early detection and immediate referral reduce complications. |
|
Kamangira, Ayele, Polite Dube, Melaku, Vushoma, (10)
|
Maternal near miss hospitalizations in the Borana Zone, Ethiopia: A facility-based longitudinal cross-sectional study |
2020 |
Ethiopia |
Maternal death or near-death occurred due to miscarriage, hemorrhage, hypertension, and infection, along with anemia, previous cesarean section, and prolonged labor. |
|
Jayaratnam, Godinho, Jennings, Thapa, (11)
|
Maternal mortality and ‘near miss’ morbidity at atertiary hospital in Timor-Leste |
2019 |
Cuba |
Thrombocytopenia and tachypnea may indicate severity, but in isolation do not suggest an immediate risk of death. |
|
Chen, Shi, Zhu, Kong, Lu, Chu, Mishu, (12)
|
Women with maternal near-miss in the intensive care unit in Yangzhou, China: a 5-year retrospective study |
2019 |
China |
Referrals from other units increase the risk of ICU admission, highlighting the need to train professionals and strengthen regional cooperation. |
|
Moudi, Arabnezhad, Ansari, Tabatabaei, (13)
|
Severe maternal morbidity among women with a history of cesarean section at a tertiary referral teaching hospital in the southeast of Iran |
2019 |
Iran |
Maternal mortality from indirect medical causes increases significantly in middle-income countries. |
|
Liyew, Worku, Afework, Essén, B.(14) |
Distant and proximate factors associated with maternal near-miss: a nested case-control study in selected public hospitals of Addis Ababa, Ethiopia |
2018 |
Ethiopia |
It is essential to plan and manage prenatal care for pregnant women with chronic hypertension, guide them during prenatal care, and strengthen maternal health services, especially in rural areas, to prevent serious complications. |
|
Woldeyes, Asefa, Muleta, (15)
|
Incidence and determinants of severe maternal outcome in Jimma University teaching hospital, south-West Ethiopia: a prospective cross-sectional study |
2018 |
Ethiopia |
Late access to obstetric care results from multiple factors; reducing delays in decision-making, access, and care can decrease the occurrence of maternal near misses and mortality. |
|
Yang, Fang, Xue Wang, Ying, Xiao-Jun, (16)
|
A retrospective cohort study of risk factors and pregnancy outcomes in Chinese pregnant women |
2018 |
China |
The MNM (Minimum Non-Mortem) rate increased with longer gestational age and premature births; ICU admission is essential to reduce mortality and improve obstetric care. |
|
Kasahun, Wako,(17) |
Predictors of maternal near miss among women admitted in Gurage zone hospitals, South Ethiopia, 2017: a case control study |
2017 |
Ethiopia |
Promoting early care is essential; in Ethiopia, community workers should raise awareness. |
|
Nakimuli, Nakubulwa, Kakaire, Osinde, Mbalinda, Nabirye, Kakande, Kaye, (18) |
Maternal near misses from two referral hospitals in Uganda: a prospective cohort study on incidence, determinants and prognostic factors |
2016 |
Afrika |
Severe pre-eclampsia was the most frequent morbidity, followed by postpartum hemorrhage; uterine rupture and eclampsia had the highest mortality rate, with ICU admission being the main near-miss criterion. |
|
Mucio, Abalos, Cuesta, Carroli, Serruya,(19)
|
Maternal near miss and predictive ability of potentially life-threatening conditions at selected maternity hospitals in Latin America |
2016 |
Uruguay |
Women with severe hypertension have a 12.8% risk of OMS, increasing to 47.5% with eclampsia or placental abruption. |
|
Lima, Amorim, Kassar, Leila Katz,(20) |
Maternal near miss determinants at a maternity hospital for high-risk pregnancy in northeastern Brazil: a prospective study |
2016 |
Brazil |
Fewer than six prenatal visits and current cesarean sections were associated with the MNM, reinforcing the importance of improving the quality of prenatal care and reducing unnecessary cesarean sections. |
|
Morais, Patz, Campanharo, Dualib, Sun, Mattar,(21)
|
Maternal near miss and potentially life-threatening condition determinants in patients with type 1 diabetes mellitus at a university hospital in São Paulo, Brazil: a retrospective study |
2016 |
Brazil |
High costs and low levels of education hinder the management of type 1 diabetes, favoring pregnancies without glycemic control; frequent prenatal care and proper insulin use are essential to prevent complications. |
|
Souza, Souza, Gonçalves,(22)
|
Determinants of maternal near miss in an obstetric intensive care unit |
2015 |
Brazil |
Hypertensive diseases, lack of prenatal care, and cesarean section were the main risk factors for near miss, highlighting the high rate of cesarean sections in Brazil (52%). |
|
Dias, Domingues, Schilithz, Pereira, Diniz, Brum, Martins, (23) |
Incidence of maternal near miss in hospital childbirth and postpartum: data from the Birth in Brazil study |
2014 |
Brazil |
Maternal near miss was more common in previous cesarean sections, forceps delivery, cesarean section without labor, and induction, and less common in vaginal delivery. |
|
Khan, Laul, Laul, Ramzan,(24) |
Prognostic factors of maternal near miss events and maternal deaths in a tertiary healthcare facility in India |
2011 |
India |
Access to and quality of care are contributing factors to maternal deaths; monitoring in the ICU can reduce deaths from serious complications. |
Source: authors (2025).
DISCUSSION
Category 1: Risk Factors for NMM Occurrence
Analysis of the manuscripts showed that gestational hypertensive diseases, prenatal failures, and previous cesarean section are important risk factors for NMM. In a Brazilian study at a tertiary maternity hospital in Campinas (SP), hypertension was associated with severe maternal morbidity in 96% of patients, with hypertensive disorders, postpartum hemorrhage, anemia, thrombocytopenia, hepatopathy, and cardiopathy being the main causes of NMM, along with factors such as time of delivery, gestational weeks, and informal examinations.(8)
Furthermore, among all the characteristics, the presence of previous chronic hypertension was the strongest risk factor for the development of NMM. Thus, women with chronic hypertension have an increased risk of several pregnancy complications, including: pre-eclampsia, placental abruption, intrauterine growth retardation, cesarean delivery, and premature birth.(9)
The finding was consistent with other studies, such as in Nigeria, which reported a seven-fold increased risk of NMM in women with pre-existing chronic hypertension, and other studies that also identified a higher risk among women with pre-existing hypertension. In Brazil, a temporal trend study between 2000 and 2014 showed an increase in the NMM ratio in the North and Northeast regions and a reduction in the South and Southeast regions, associated with better obstetric care and greater socioeconomic development.(12)
In addition, hypertensive complications were the most frequent in the maternity hospitals surveyed, and this is also the main cause of maternal illness and death in Brazil and in several countries in Africa, Asia, Latin America and the Middle East.(16) Hypertensive pathologies, when identified early and managed adequately during prenatal care, decrease the likelihood of triggering serious complications during the pregnancy-puerperal cycle.
Furthermore, an association was observed between severe maternal morbidity and the fact that the woman was classified as a risk group, an expected relationship, but one that shows the need for analysis of obstetric risk at each prenatal visit, not a rigid classification to be performed only at the first moment of pregnancy. Furthermore, an association was observed between severe maternal morbidity and induced labor and high-risk pregnancy, with such associations found in studies conducted in Brazil and Australia.(21,23)
It is worth noting that, regarding the main direct obstetric causes of NMM in the ICU, they were hypertensive disorders of pregnancy and PPH, while the indirect obstetric causes of NMM cases admitted to the ICU were heart disease. In parallel, outside the ICU, the most common direct obstetric cause was PPH, followed by hypertensive diseases of pregnancy.
The main cause of PPH in both groups was placental accumulation/placenta previa. Among ICU admissions, 77.27% presented postoperative complications, whether due to hemorrhagic complications, respiratory compromise, cardiac instability, sepsis, or pulmonary edema. The ratio between near miss and maternal mortality in the same study was 7.33:1, meaning that for every 7 near misses with ICU admissions, one case of maternal mortality was observed.(21)
Furthermore, an association was found between parity and NMM, with multigravida and nulligravida women presenting more complications compared to other maternal groups. It was also observed that women with a history of anemia have a higher chance of near-miss maternal events than those without a previous history of anemia. Untreated anemia can cause postpartum hemorrhage (PPH) and hypovolemic shock and is a common cause of adverse maternal outcomes.(13)
Some studies have pointed to PPH as the main cause of maternal deaths and near-miss events, consistent with the literature that indicates PPH and pre-eclampsia as the main overall causes of maternal mortality and morbidity.(17) In addition, referral from another unit was a significant risk factor for ICU admission, highlighting the need to strengthen the training of primary care professionals and the implementation of timely referrals.
Regional cooperation between professionals at lower levels should be reinforced, as women referred from other units have a higher risk of NMM, especially due to serious complications and transportation difficulties. Improving access, the referral system, and decentralization of maternal care can reduce these events. Even after the referral decision, many women are transferred without treatment being initiated, and seeking care in poorly equipped units causes significant delays, contributing to NMM.(7)
Therefore, early detection and better blood pressure control with immediate referral of pre-eclampsia cases to tertiary centers and timely termination of these pregnancies can reduce complications and near-miss events.
Category 2: Sociodemographic and Contextual Factors
Severe maternal morbidity involves sociodemographic and care factors, and understanding this relationship is crucial, as maternal outcome depends on the social determinants of health, such as access to services and social protection. Humanitarian crises, conflicts, lack of supplies and professionals, gender inequality, and the absence of protective policies increase the risk of maternal mortality and MMR in certain regions.(6,19)
In this context, 42% of studies found no relationship between severe maternal morbidity and sociodemographic variables, common in countries in phase III of obstetric transition, such as Brazil, with MMR between 50 and 299 deaths per 100,000 live births. Studies from China and India also showed no significant association, while maternal deaths in these countries are more linked to the quality of obstetric care.(11) In contrast, research in Ethiopia, Uganda, Brazil, and Iran showed the influence of sociodemographic determinants.
Regarding the influence of age range on MNM, some literature indicates the extremes of reproductive age as a risk factor.(7) The “Born in Brazil” survey (2013) showed a predominance of MNM in adolescents (10–14 years) and in women over 35 years of age.(23) A study in seven Latin American countries showed a similar pattern.(19) Predominantly, age ≥35 years showed a significant association with MNM.(6-7,11,20) However, most manuscripts included women between 20 and 35 years of age.(4,5,15,18,20,22)
Furthermore, the level of education is a fundamental social determinant in the investigation of maternal outcome. Low educational attainment can make pregnant women less informed about important care during the natal and perinatal period, which increases the chances of lower attendance at prenatal appointments, failure to abandon harmful behaviors, and disregard for warning signs during pregnancy, along with failure to seek timely healthcare services.(5,22)
In view of this, a relationship was found between few years of schooling and NMM.(5,7,13,18,22) It is noteworthy that in 68% of the studies that stratified the sociodemographic profile, women affected by NMM had a low level of education; however, only three manuscripts showed statistical significance when correlating the variable with maternal outcome. In contrast, in a Brazilian study, there was a predominance of women with NMM who had completed higher education.(20)
Regarding marital status, studies predominantly indicated married women as the most affected by MNM. It is emphasized that marital status has a significant impact on maternal outcome because it reflects the absence of emotional, financial, or social support during the pregnancy-puerperal cycle.(15,20)
Another factor with a major influence on maternal morbidity and mortality is skin color. Sociodemographic profile investigations revealed a predominance of MNM in non-white women.(6,19,20,22) Brazilian research that aimed to analyze the ethnic patterns of maternal morbidities in the North and Northeast regions showed that the occurrence of MNM was higher among indigenous and black women than among white women.(24)
Furthermore, other factors that impact maternal outcome include: low income, residing in the periphery or rural areas, having had few prenatal consultations, and the occurrence of any delay in receiving care. Given this, the absence of prenatal care or the attendance of few consultations was a prevalent characteristic in the manuscripts that investigated this history. Lima et al. found an association between NMM and having had fewer than six prenatal consultations.(11,15,20)
Furthermore, residing in remote locations compromises attendance at prenatal consultations due to the challenges related to travel. A study conducted by Souza et al. demonstrated that residing in rural areas is positively associated with the occurrence of near misses.(22,24)
Similarly, distance compromises timely decision-making, creating a problem that influences financial, geographical, and structural factors.(5,20) It should be noted that a large proportion of the manuscripts reported some delay in providing care to pregnant women. Most were associated with the first delay, which refers to the delay in seeking health services after the onset of any complaint.(7,11,20)
Women who remained at home for more than 4 hours after the onset of the complication had 2.8 times greater risk of developing NMM than women who sought health care earlier. It is noteworthy that the delay in seeking health care is mainly due to the disregard of symptoms as a warning sign and the negative influence of the partner or family members on the woman's decision to seek health care.(11,14,20)
Therefore, delay in the treatment of obstetric complications worsens the situation, increasing the risk of unfavorable outcomes. The acute severity of these complications reinforces the importance of pregnant women seeking and accessing health care early, with maternal education being fundamental to reducing serious events.
Category 3: Interrelationship between near miss and cesarean delivery
A priori, cesarean section is a surgical procedure that involves blood loss, anesthetic risks, and increases the risk of postoperative complications. Therefore, it appears that a cesarean section is a risk factor that increases the risk of complications. Studies are controversial on how cesarean section in the current pregnancy contributes to near miss cases.(14,24)
Furthermore, the incidence of cesarean sections continues to increase worldwide and reached 55% in Brazil in 2016. Thus, cesarean section in the current pregnancy had a high incidence in the group of pregnant women with NMRs (80%) and was significantly associated in the multivariate analysis, in which it increased the risk of NMR occurrence fivefold. This finding corroborates the results of other studies.(14)
However, this association may be affected by confounding factors. In low-risk pregnancies, cesarean sections are known to pose potential health risks to women and may be a modifiable risk factor for maternal mortality when compared to vaginal delivery due to increased thromboembolism, puerperal infection, hemorrhage, and anesthetic complications.(2)
Regarding obstetric history and characteristics of the current pregnancy, a higher incidence of maternal near miss was observed in women with previous cesarean sections, with an increase in the incidence of maternal near miss as the number of previous cesarean sections increased. Cesarean delivery was associated with ICU admission, similar to a study from Italy, and may increase the risks of bleeding and sepsis, leading to hysterectomy and longer hospital stays, but may also be a protective factor against adverse outcomes.(3,8)
In a study of approximately 370,000 women in the Netherlands, the risk of near miss was 5.2 for those who had a previous cesarean section and 5.9 for those undergoing a current elective cesarean section, demonstrating that the procedure increases the likelihood of severe maternal morbidity and complications such as infection, hemorrhage, and thromboembolism.(1) It is noteworthy that, in line with previous studies conducted in Southern Ethiopia, in the Tigray region and in West Arsi, it was also found that women with a previous history of cesarean section (CS) were more prone to maternal near miss events (AOR = 3.70, 95% CI: 1.42–9.60). A prospective cohort study in Northeast Brazil also indicated that cesarean section was significantly associated with the occurrence of maternal near misses. (1,25)
Although it saves the lives of a woman and a newborn, a previous history of cesarean section increases the risk of hemorrhage, recurrence, placental accumulation in scar tissue, thromboembolism, uterine rupture during attempted vaginal delivery after cesarean section, and other complications, which could increase the likelihood of MNM. We believe that further studies should be conducted to clarify the benefits and risks of the optimal level of cesarean sections to protect the mother and fetus in high-risk pregnancies.(25)
FINAL CONSIDERATIONS
The analysis of the selected studies allowed the identification of some factors that may be related to risk factors for the occurrence of maternal near misses (NMM) among pregnant women or in the immediate postpartum period. However, it is important to highlight some limitations of the study, since there is still a scarcity of recent studies that focus precisely on near misses and their maternal complications.
It was observed that chronic hypertension, rural residence, absence of prenatal care, and previous anemia were factors associated with maternal near misses. Hypertensive disorders of pregnancy and postpartum hypertension (PPH) were the main causes of NNM in the NICU, indicating the need to improve the training of primary care professionals and encourage vaginal delivery when there is no indication for cesarean section.
Furthermore, sociodemographic level, in turn, constitutes an essential social determinant in the analysis of maternal outcomes. Because existing limitations regarding education level, ethnicity, access to transportation, low income, and marital status can compromise a pregnant woman's access to important information about necessary prenatal and perinatal care, leading to lower adherence to prenatal appointments, the continuation of established habits, and a lack of recognition of warning signs during pregnancy.
It is worth noting that although a previous cesarean section can save the life of a woman and a newborn, it also increases the risk of complications such as hemorrhage, recurrence of problems, placental adhesion to scar tissue, thromboembolism, uterine rupture during an attempt at vaginal delivery after cesarean section, among others. These factors can significantly increase the likelihood.
Therefore, it is crucial to encourage early seeking of healthcare; in Ethiopia, health extension workers should be strengthened to increase community awareness. Women with a history of cesarean section require special attention from family members and professionals to prevent serious obstetric complications.
Therefore, it is clear that there are several risk factors for the occurrence of NMM (Neuromyalgia Mucosal) among pregnant women or in the immediate postpartum period. Given this, healthcare professionals and institutions should pay closer attention to early detection and blood pressure control, with immediate referral of pre-eclampsia cases to tertiary centers and timely termination of these pregnancies, as these factors can reduce complications and near-miss events.
REFERENCES
1. United Nations. Development Goals The Millennium. New York: United Nations; 2007.
2. Fundação Oswaldo Cruz. Instituto Nacional de Saúde da Mulher, da Criança e do Adolescente Fernandes Figueira. Portal de Boas Práticas em Saúde da Mulher, da Criança e do Adolescente. Postagens: Tendências na Mortalidade Materna 2000-2020. Rio de Janeiro: Fiocruz; [s.d.].
3. Organização Mundial da Saúde (OMS). Avaliando a qualidade dos cuidados para complicações graves na gravidez: a abordagem de quase acidente da OMS para a saúde materna. Genebra: OMS; 2011.
4. Chhavi G, Suri J, Bachani S, Bharti R, Mittal P. Carle’s obstetric early warning score as a screening tool for critical care admission. India. 2023.
5. Teshome HN, Ayele ET, Hailemsekel S, Yimer O, Mulu GB, Tadese M. Determinants of maternal near-miss among women admitted to public hospitals in North Shewa Zone, Ethiopia: a case-control study. Ethiopia. 2022.
6. Andrade MS, Bonifácio LP, Sanchez JAC, Ciabati LO, Zaratini FS. Factors associated with serious maternal morbidity in Ribeirão Preto, São Paulo State, Brazil: a cross-sectional cohort study. Brazil. 2022.
7. Tenaw SG, Assefa N, Mulatu TT, Tura AK. Maternal near miss among women admitted in major private hospitals in Eastern Ethiopia: a retrospective study. Ethiopia. 2021.
8. Luna JMB, Rúa DMP, Ordoñez IR, Fernández PA, Vidarte MFE. Description of criteria for near miss in high-complexity obstetric population with sickle cell anemia: an observational study. Brasil. 2020.
9. Krishna Kumar MK, Joshi A, Saraswat M, Jose T, Kapoor R, Saha M. Near‐Miss Incidents in Obstetric Patients Admitted to an Intensive Care Unit of a Tertiary Care Center in Eastern India: A Retrospective Cohort Study. Índia. 2020.
10. Kamangira B, Ayele G, Dube PP, Melaku K, Vushoma E. Maternal near miss hospitalizations in the Borana Zone, Ethiopia: a facility-based longitudinal cross-sectional study. Ethiopia. 2024.
11. Jayaratnam S, Godinho MLF, Jennings B, Thapa AP. Maternal mortality and ‘near miss’ morbidity at a tertiary hospital in Timor-Leste. Cuba. 2019.
12. Chen Y, Shi J, Zhu Y, Kong X, Lu Y, Chu Y, Mishu MM. Women with maternal near-miss in the intensive care unit in Yangzhou, China: a 5-year retrospective study. China. 2019.
13. Moudi Z, Arabnezhad L, Ansari H, Tabatabaei SM. Morbidade materna grave entre mulheres com histórico de cesariana em um hospital universitário terciário de referência no sudeste do Irã. Public Health. 2019.
14. Liyew EF, Yalew AW, Afework MF, Essén B. Incidência e causas de quase acidente materno em hospitais selecionados de Adis Abeba, Etiópia. PLoS One. 2017.
15. Woldeyes WS, Asefa D, Muleta G. Incidence and determinants of severe maternal outcome in Jimma University teaching hospital, South-West Ethiopia: a prospective cross-sectional study. Ethiopia. 2018.
16. Yang Y, Fang Y, Xue Wang X, Ying Z, Xiao-Jun L, Yin Z. A retrospective cohort study of risk factors and pregnancy outcomes in Chinese pregnant women. China. 2018.
17. Kasahun AW, Wako WG. Predictors of maternal near miss among women admitted in Gurage zone hospitals, South Ethiopia, 2017: a case control study. BMC Pregnancy Childbirth. 2017.
18. Nakimuli A, Nakubulwa S, Kakaire O, Osinde MO, Mbalinda SN, Nabirye RC, et al. Maternal near misses from two referral hospitals in Uganda: a prospective cohort study on incidence, determinants and prognostic factors. Africa. 2016.
19. Mucio B, Abalos E, Cuesta C, Carroli G, Serruya S. Maternal near miss and predictive ability of potentially life-threatening conditions at selected maternity hospitals in Latin America. Uruguay. 2016.
20. Lima THB, Amorim MM, Kassar SB, Katz L. Maternal near miss determinants at a maternity hospital for high-risk pregnancy in northeastern Brazil: a prospective study. Brazil. 2019.
21. Morais LR, Patz BC, Campanharo FF, Dualib PM, Sun SY, Mattar R. Maternal near miss and potentially life-threatening condition determinants in patients with type 1 diabetes mellitus at a university hospital in São Paulo, Brazil: a retrospective study. Brasil. 2016.
22. Souza MAC, Souza THSC, Gonçalves AKS. Determinants of maternal near miss in an obstetric intensive care unit. Brazil. 2015.
23. Dias MAB, et al. Incidência do near miss materno no parto e pós-parto hospitalar: dados da pesquisa Nascer no Brasil. Cad Saude Publica. 2014.
24. Khan T, Laul P, Laul A, Ramzan M. Prognostic factors of maternal near miss events and maternal deaths in a tertiary healthcare facility in India. India. 2017.
25. De Lima THB, et al. Determinantes do near miss neonatal em uma maternidade de gestação de alto risco no Nordeste do Brasil: um estudo prospectivo. BMC Pregnancy Childbirth. 2018.
Funding and Acknowledgments:
This research received no funding.
Authorship Criteria (Author Contributions)
Jeane Araújo Costa: conception and design of the study, data collection, analysis and interpretation, manuscript writing.
Natália Pereira Marinelli: guidance, critical review of intellectual content and approval of the final version.
Layana Pachêco de Araújo Albuquerque: contribution to data analysis, critical review and methodological adequacy.
Kélvya Fernanda Almeida Lago Lopes: collaboration in the discussion of results and final review of the manuscript.
Conflict of Interest Statement
“Nothing to declare”.
Data Availability Statement
No databases were generated in this study. The information presented is described in the body of the article.
Scientific Editor: Ítalo Arão Pereira Ribeiro. Orcid: https://orcid.org/0000-0003-0778-1447
Rev Enferm Atual In Derme 2026;100(1): e026029
![]()